
Top Ten Cancers in the Greater Bay Area: Incidence and Mortality,1988-2021
In our 2024 report, the Greater Bay Area Cancer Registry highlights the top ten cancers in the nine Bay Area counties of its region. We provide an overview of cancer incidence and mortality in the Greater Bay Area, and downloadable data sheets for each of the top ten cancer sites. For interactive graphics showing incidence and mortality for the most common cancers, please use the GBACR Dashboard.
Incidence and Mortality in the Greater Bay Area, 1988-2021
Rates of invasive cancers have decreased significantly during the 34-year period from 1988 through 2021 in the Greater Bay Area. Significant declines were also noted by the American Cancer Society in their Annual Cancer Statistics report [1].
Last year, we reported that we observed 9.6% and 9.3% fewer cancer cases diagnosed among males and females in 2020, respectively, compared to expected counts calculated from previous years. These estimates were impacted by the COVID-19 pandemic and the limited access to cancer-related healthcare services throughout the United States. Starting in 2023, SEER recommended excluding the 2020 incidence data from the estimation of trends (see Impact of COVID on the April 2023 SEER Data Release). As a result, trends for incidence exclude the 2020 data point (rate). The 2021 cancer case counts are aligned with expectations prior to 2020.
The five most common invasive cancers—breast, prostate, lung and bronchus, colorectal, and uterine—accounted for slightly over half of all newly diagnosed cancers in the Greater Bay Area. Lung and bronchus, breast, prostate, colorectal, and pancreatic cancers were the most common cause of cancer deaths, collectively accounting for half of all cancer deaths in the Greater Bay Area.
Incidence and Mortality Trends Over Time
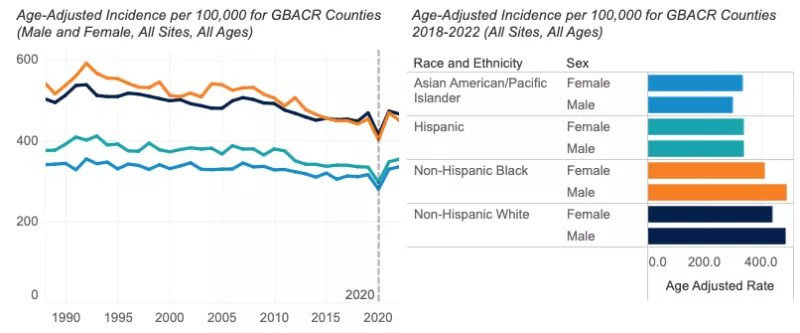
- Since 1988, yearly incidence of invasive cancer has declined more among males (-0.9%) than females (-0.2%). This is driven largely by declines in the incidence of smoking-related cancers (e.g., lung and bronchus) and prostate cancer in males. In more recent years, since 2013, incidence among males and females has been stable (excluding the 2020 incidence rate for calculation of recent trends).
- As with incidence, a significant annual decline has occurred for mortality since 1988 (males: -2.0%; females: -1.7%). In more recent years, from 2011 through 2021, males and females combined cancer mortality declined by -2.3% per year. Trends were comparable when looking at males and females separately.
Incidence, 2017-2021
- In 2021, 35,298 invasive cancers were diagnosed in the Greater Bay Area.
- The incidence of all invasive cancers from 2017-2021 was higher in males than females.
- Males: incidence was highest among NH Black males (466.6 per 100,000), followed by NH White (464.2 per 100,000), Hispanic (340.2 per 100,000), and AANHPI males (283.1 per 100,000).
- Females: NH White females had the highest cancer incidence (425.4 per 100,000), followed by NH Black (388.9 per 100,000), Hispanic (327.7 per 100,000), and AANHPI (312.8 per 100,000) females.
- Among Greater Bay Area counties, Santa Cruz County had the highest overall cancer incidence among males and females combined (457.0 per 100,000), followed by Marin County (437.6 per 100,000), driven by higher incidence of female breast cancer and melanoma, particularly among males.
- Cancer incidence among males was significantly lower in the Greater Bay Area than California overall (405.5 vs. 414.2 per 100,000). Among females, overall cancer incidence was similar between the Greater Bay Area and all of California (379.0 vs. 380.8 per 100,000, respectively).

Mortality, 2017-2021
- In 2021, 10,421 cancer deaths occurred in the Greater Bay Area.
- Cancer mortality from 2017-2021 was higher in males than females.
- Males: mortality was highest among NH Black males (199.1 per 100,000), followed by NH White (145.5 per 100,000), Hispanic (126.5 per 100,000), and AANHPI males (110.7 per 100,000).
- Females: NH Black females had the highest cancer mortality (146.8 per 100,000), followed by NH White (111.6 per 100,000), Hispanic (97.4 per 100,000), and AANHPI (83.3 per 100,000) females.
- From 2017 through 2021, overall cancer mortality in the Greater Bay Area was significantly lower than California for both males (138.2 vs. 157.4 per 100,000) and females (105.2 vs. 117.6 per 100,000)
Data Tables - All Cancer Sites
References
[1] Siegel, R. L., K. D. Miller, N. S. Wagle, and A. Jemal. "Cancer Statistics, 2024." CA Cancer J Clin 74, no. 1 (Jan 2024): 12-49. https://doi.org/10.3322/caac.21820