Top Ten Cancers in the Greater Bay Area: Incidence and Mortality,1988-2022
In our 2025 report, the Greater Bay Area Cancer Registry describes incidence and mortality for the top ten cancers in the nine Bay Area counties of its region. Downloadable data sheets for each of the top ten cancer sites are provided (data for additional cancer sites are available upon request to [email protected]).
Incidence and Mortality in the Greater Bay Area, 1988-2022
Overall rates of invasive cancers have decreased during the 35-year period from 1988 through 2022 in the Greater Bay Area. Significant declines were also noted by the American Cancer Society in their 2025 Annual Cancer Statistics report [1].
After reporting an approximate 9.5% fewer cases in 2020 due to the reduction in screening and diagnosis with the COVID-19 pandemic, we continue to see the number of cancer cases diagnosed aligned with expectations prior to 2020. In fact, we report a slight increase in the number of cancer cases since 2021, while deaths due to cancer continue to fall in the Greater Bay Area. The recent increase in incidence may be attributable to cancers diagnosed at a later stage. Breast (female invasive) and prostate cancers are likely driving this trend. For distant stage female breast cancer, we report a significant increase in incidence at 8.1% per year since 2019. For prostate cancers diagnosed at distant stage, we report a significant 6.0% increase per year since 2010. Recent increases in distant stage for these cancers have been reported nationally and statewide for California [2, 3, 4].
The five most common invasive cancers—breast, prostate, lung and bronchus, colorectal, and uterine—accounted for half (50.5%) of all newly diagnosed cancers in the Greater Bay Area. Lung and bronchus, breast, prostate, colorectal, and pancreatic cancers were the most common cause of cancer deaths, collectively accounting for slightly less than half (47.8%) of all cancer deaths in the Greater Bay Area from 2018 to 2022.
Incidence and Mortality Trends Over Time
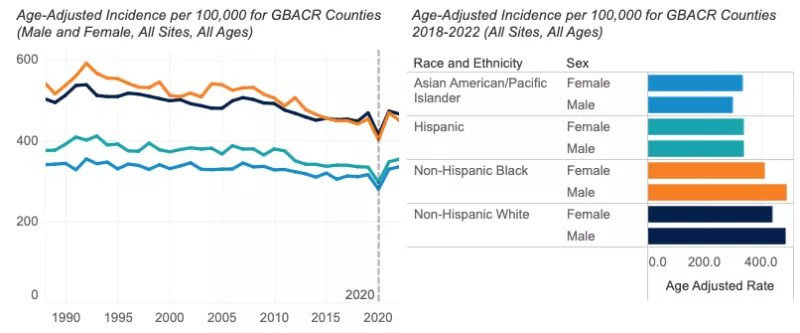
- Since 1988, yearly incidence of invasive cancer has declined more among males (-0.7%) than females (-0.1%). This is driven largely by declines in the incidence of smoking-related cancers (e.g., lung and bronchus) and prostate cancer in males. In recent years, since 2016, incidence among females has increased by 1.2% per year, while remaining stable among males.
- A significant annual decline has occurred for cancer mortality since 1988 (males: -2.0%; females: -1.7%). This is likely due to a combination of factors, including advancements in treatment, continued increased screening, and the effects of a continued reduction in smoking behavior.
Incidence, 2018-2022
- In 2022, 37,139 invasive cancers were diagnosed in the Greater Bay Area.
- The incidence of all invasive cancers from 2018-2022 was higher in males (420.3 per 100,000) than females (394.1 per 100,000).
- Males: Incidence was highest among NH Black males (487.7 per 100,000), followed by NH White (483.4 per 100,000), Hispanic (340.3 per 100,000), and AANHPI males (299.3 per 100,000).
- Females: NH White females had the highest cancer incidence (437.7 per 100,000), followed by NH Black (411.3 per 100,000), Hispanic (338.1 per 100,000), and AANHPI (333.8 per 100,000) females.
- Among Greater Bay Area counties, Santa Cruz County had the highest overall cancer incidence among males and females combined (462.6 per 100,000), followed by Marin County (455.3 per 100,000). This appears to be driven by higher incidence of female breast cancer and melanoma (particularly among males). Alameda County had the lowest overall cancer incidence rate (380.2 per 100,000).
- Cancer incidence among males was lower in the Greater Bay Area than California overall (420.3 vs. 427.6 per 100,000). Among females, overall cancer incidence was similar in the Greater Bay Area when compared to all of California (394.1 vs. 391.3 per 100,000, respectively).

Mortality, 2018-2022
- In 2022, 10,286 cancer deaths occurred in the Greater Bay Area.
- Cancer mortality from 2018-2022 was higher in males (137.2 per 100,000) than females (104.9 per 100,000).
- Males: Mortality was highest among NH Black males (202.4 per 100,000), followed by NH White (144.9 per 100,000), Hispanic (120.9 per 100,000), and AANHPI (111.3 per 100,000) males.
- Females: NH Black females had the highest cancer mortality (149.6 per 100,000), followed by NH White (111.7 per 100,000), Hispanic (93.9 per 100,000), and AANHPI (83.8 per 100,000) females.
- From 2018 through 2022, overall cancer mortality in the Greater Bay Area was significantly lower than California for both males (137.2 vs. 155.8 per 100,000) and females (104.9 vs. 117.4 per 100,000).
Data Tables - All Cancer Sites
References
[1] American Cancer Society. Cancer Facts & Figures 2025. Atlanta: American Cancer Society; 2025.
[2] Hendrick, R. E. and D. L. Monticciolo (2024). "Surveillance, Epidemiology, and End Results Data Show Increasing Rates of Distant-Stage Breast Cancer at Presentation in U.S. Women." Radiology 313(3): e241397.
[3] Giaquinto, A. N., H. Sung, L. A. Newman, R. A. Freedman, R. A. Smith, J. Star, A. Jemal and R. L. Siegel (2024). "Breast cancer statistics 2024." CA Cancer J Clin 74(6): 477-495.
[4] Van Blarigan, E. L., M. A. McKinley, S. L. Washington, 3rd, M. R. Cooperberg, S. A. Kenfield, I. Cheng and S. L. Gomez (2025). "Trends in Prostate Cancer Incidence and Mortality Rates." JAMA Netw Open 8(1): e2456825.